- The TriDoc Podcast-in Supplement form
- Posts
- Episode 191-Labral tears of the shoulder/Dr.Kevin Stone
Episode 191-Labral tears of the shoulder/Dr.Kevin Stone
A brief synopsis of the episode's main discussions and takeaways as well as extended references
Jeff Sankoff
February 27, 2026
A common injury amongst swimmers, can labral tears be rehabilitated conservatively or is surgery the only option for those who have them?
Table of Contents
Labral Tears of the shoulder-The MMB looks at options for treatment and prognosis for return to sport
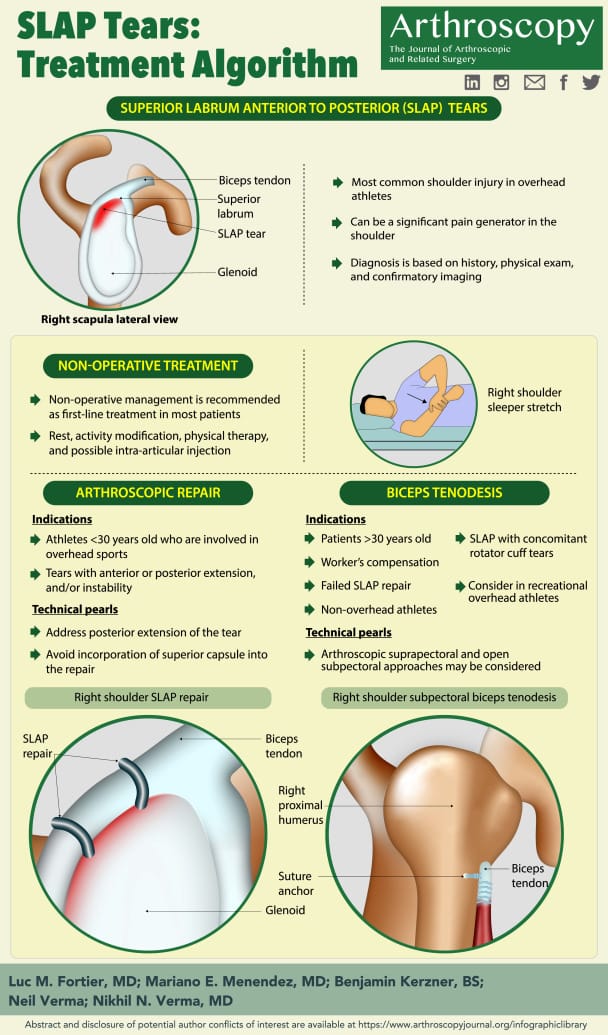
A shoulder labral tear involves injury to the fibrocartilaginous rim that deepens the glenoid socket and stabilizes the humeral head. Tears are commonly classified as SLAP (superior labrum anterior-posterior) lesions, anterior/inferior Bankart-type tears, or posterior labral tears. Management depends on tear type, mechanism, instability, sport demands, and patient age. On this episode’s MMB we looked at the evidence supporting different approaches and examined what the prognosis is for returning to sport.
Nonoperative management is first-line for many athletes, particularly with SLAP and posterior tears without frank instability. Treatment includes activity modification, short-term anti-inflammatories, and a structured physical therapy program emphasizing scapular stabilization, rotator cuff strengthening, posterior capsule mobility, and kinetic chain mechanics. Many athletes improve with 3–4 months of rehabilitation, especially non-overhead athletes. Obviously, this is not the case for swimmers!
Surgical management is considered for persistent pain, recurrent instability, or failure of rehab. Arthroscopic techniques include labral repair (using suture anchors), capsular plication, or biceps tenodesis (commonly for type II SLAP tears in older athletes). Postoperative rehab is staged: sling immobilization (2–4 weeks), progressive range of motion, strengthening by 8–12 weeks, and sport-specific progression after 3–4 months.
Return to sport (RTS) prognosis varies by sport and tear type. Overall RTS rates after arthroscopic repair are approximately 70–90%. Overhead (swimming) and throwing athletes have more variable outcomes after SLAP repair, with elite baseball pitchers showing lower rates of return to prior performance. Biceps tenodesis may yield more reliable pain relief in athletes over 30.
Time to full RTS typically ranges from 4–6 months for non-throwing sports and 6–9 months for overhead or contact sports. Prognosis is best with early diagnosis, absence of significant bone loss, adherence to rehabilitation, and realistic expectations regarding performance level.
Dr. Kevin Stone returns to talk about advances in orthopedics
About Dr. Stone: Dr. Kevin Stone is an orthopaedic surgeon at The Stone Clinic and also the chairman of the Stone Research Foundation in San Francisco, California who lectures around the world as an expert in cartilage and meniscal growth, replacement, and repair, with over 40 U.S. patents on novel inventions to improve healthcare.
In this episode, we dive deep into the world of orthopedic advancements with Dr. Kevin Stone, who shares some wild stats from a recent study where older adults faced the dreaded knee replacement but came out with a new lease on life thanks to meniscus grafts. Picture this: 42% of these patients enjoyed 8.5 years of relief before even considering joint replacements. Meanwhile, the rest? They just decided to stick around and never need a replacement at all. How's that for buying some time? What really stands out, though, is the idea that even if your knee's been through the wringer, there's hope. Dr. Stone talks about giving patients a shock absorber to help them get back to their favorite sports and activities. So, if you've ever thought your athletic days were over because of a crummy knee, think again! We’re talking about athletes returning to sport better than ever, thanks to these new innovations. This episode is basically a pep talk for anyone who's ever felt like their body has betrayed them, reminding you that with the right treatment, you could be back out there, living your best athletic life.
Episode takeaways:
In a groundbreaking study, 42% of patients aged 50 and above found relief from knee pain for over eight years after receiving a meniscus replacement, avoiding joint surgery.
Even in advanced arthritis cases, innovative orthopedic techniques can provide athletes with much-needed shock absorption, helping them stay active longer than ever before.
Dr. Kevin Stone emphasizes that surgery isn't always the best solution; sometimes aggressive physical therapy can yield better results without the need for invasive procedures.
References used for the MMB
Shoulder anatomy (Ladd et al., 2021)
The glenohumeral joint: “golf ball on a tee.” Ball-and-socket joint that maximizes range of motion leads to inherent instability.
Labrum tear types (Manske & Prohaska, 2010)
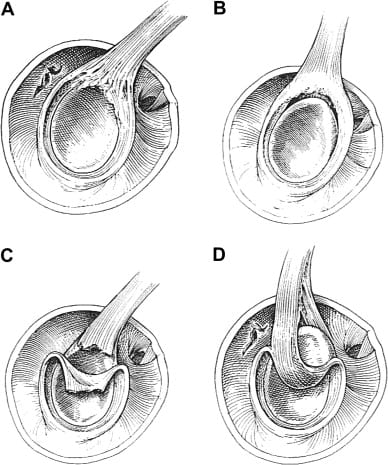
Type I labrum tear. Fraying and/or degenerative labrum attachment to glenoid rim, but contact is maintained.
Type II labrum tear, a.k.a. SLAP tear. Detachment of the superior biceps–labral complex attachment from the glenoid rim. This labrum tear location can include fraying, but is differentiated from type I by the presence of detachment. This is the most common labrum tear among overhead athletes by far.
Type III labrum tear. Bucket-handle tear of the labrum with an intact biceps anchor at the glenoid rim.
Type IV labrum tear. Bucket-handle tear where the tear extends into the biceps tendon.
Labrum tears can exist with tears of the anteroinferior labrum, called Bankart lesions (Lee et al., 2018), or humeral head compression fractures, called Hill Sach's lesions (Pak & Kim, 2025). Concurrent tears will alter treatment plans.
PRP review that says in most cases it is not helpful: https://pmc.ncbi.nlm.nih.gov/articles/PMC10155124/
Platelet-rich plasma (PRP) has no established role in the treatment of SLAP tears, as the available medical literature does not address PRP specifically for this indication. The existing evidence on PRP in shoulder pathology focuses primarily on rotator cuff tendinopathy, partial-thickness rotator cuff tears, and rotator cuff repair augmentation
Course of Treatment
Conservative management first: Emphasize rotator cuff and scapular stabilizer strength/endurance, posterior shoulder stretching to restore full, symmetrical internal rotation, and relative rest from aggravating activities. Address capsular/cuff tightness, postural or cervicothoracic impairments, and any distal referral sources contributing to shoulder symptoms. If symptoms persist, consider anti-inflammatory treatment or corticosteroid injection; unresolved cases may require diagnostic ar
Describes a systematic review of outcomes given biceps tenodesis, an alternative surgery for GHL
In-season return to play may be possible with conservative care, long-term satisfaction and shoulder stability in young athletes with recurrent posttraumatic instability typically require surgical stabilization.
A 6–8 week exercise program emphasizing shoulder external rotator and scapular retractor strengthening plus pectoral stretching reduces shoulder pain incidence in swimmers; combining exercise with manual therapy helps manage existing pain.
Dry-land and open kinetic chain exercises better improve shoulder strength/endurance than water-based or closed-chain training, though longer programs (>12 weeks) improve strength metrics without clear pain reduction—results should be applied cautiously due to study limitations.
SLAP lesions are common in overhead/throwing athletes; initial management is typically conservative, with a recent shift away from SLAP repair toward procedures like biceps tenodesis as surgical indications narrow.
Type I & III lesions are usually treated with arthroscopic debridement and early ROM, while Type II/IV repairs follow a phased rehab (initial protection, delayed biceps loading, progressive ROM/strengthening) with return to play around 6–9 months; biceps tenodesis requires prolonged biceps protection (~10 weeks).
Despite common elements (e.g., ~4 weeks sling use, goal of full ROM by 12 weeks), rehab protocols show high variability, inconsistent return-to-sport guidance, and limited adjustment for biceps tenodesis—highlighting the need for standardized, sport-specific protocols.
Shoulder injury type was not associated with swimming stroke; most swimmers showed normal scapular rhythm, impingement cases returned to swimming with nonoperative care (~1.6 months), while labral tears required arthroscopic repair with return at ~2.9 months, highlighting the importance of accurate diagnosis and appropriate treatment selection.
From 22 included studies, there was no strong evidence linking most assessed variables to shoulder pain or injury in competitive swimmers; moderate evidence supported associations with competitive level (nondirectional) and shoulder muscle recruitment patterns, while ROM, strength ratios, training frequency, stroke specialty, and demographics were not associated.
Shoulder strength-endurance and workload management (e.g., high acute-to-chronic load ratios) appear the most relevant modifiable risk factors; swimmers with prior injury are at high risk of reinjury, whereas ROM and maximal strength are unlikely predictors.
Outcomes (Steinmetz et al., 2022)
Meta-analysis of 5 studies (combined n=244).
Nonsurgical outcomes: Overall return-to-sport rate was just over 50%, with return to prior performance just over 40%; athletes completing full rehab had much higher success (78% return to play). Anywhere from 10 weeks to 3 months PT
Surgical outcomes: Reported return-to-play rates ranged from 20–100%, with systematic reviews showing an average of ~79.5% return to play.
Not a subscriber to the podcast? Click here!
Support the podcast: TriDoc Podcast Patreon site
Need an endurance coach? TriDoc Coaching
Reply